
 Facebook
Facebook Twitter
Twitter LinkedIn
LinkedIn Forward
ForwardAnatomic Landmarks
TBD
Equipment
TBD
Technique Steps
Preoperative evaluation for intraoperative strategy
Aortic control techniques: Clampless
Surgical identification of lumbar arteries
Retention of endograft
Securing of endograft
Omental flap to fill aneurysm sac
Technique video
Technique
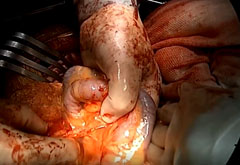
Mobilizing the duodenum
The proximal and distal seals were evaluated to determine that they were adequate. The approach is similar to an open aneurysm repair. Because the seals were determined to be adequate, the aneurysm was opened and was not clamped proximally or distally.

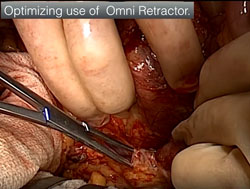
Optimize the use of the omni retractor
The omni retractor is key to the wide mobilization of the duodenum. In many cases, the renal vein is divided in order to access the neck. If it is possible to save the renal vein, that should be done.
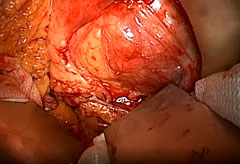
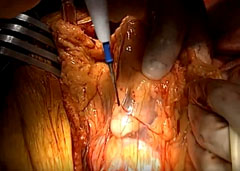
Exposing the aneurysm sac
Splanchnic blades provide excellent neck exposure. The renal artery retractor is shown below. The renal neck is exposed and shown below, demonstrating a very large aneurysm. The omni blades are key to open aortic procedures and, in this case, to provide adequate exposure proximally.
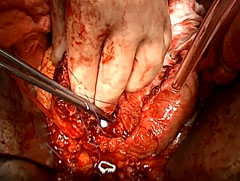
The neck is exposed and dissected proximally. The iliacs are exposed proximally and distally, and the aneurysmal sac is opened. At this point, there is no proximal or distal control, but the exposure is such that clamps can be placed, if they are needed.
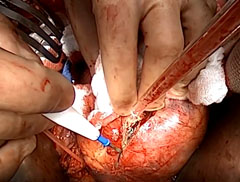
The aneurysm sac is under a remarkable degree of pressure, so it is "T-d" off proximally and distally, and the aneurysm sac is entered. The exudate is cleared out and cultured. It is important not to extend the proximal iliac (?) artery all the way up to the clamp (if a clamp is needed). The aneurysm sac is cleaned and cleared of any embedded devices, and the clot is removed.
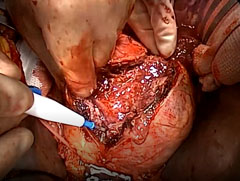

Any breaches in the lumbar vessels are repaired.

Check for residual clot all around the endograft (arrow).

Closure
The walls of the aneurysm sac are oversewn and the seal zone is evaluated. Often, two to three (pegited?) sutures are placed through the aneurysm up through the neck of the aorta both proximally and distally.

A retatum (?) and alimental flap is taken down in a retrocolic position and packed inside of the aneurysm sac.
Pearls
Percutaneous interventions for type 2 endoleaks may fail
the 1-2 lumbar arteries alone can cause sac enlargement
Open salvage techniques are necessary
Endograft replacement is not necessary in select cases
References
1. TBD
2. TBD